Articles
Assessing Global Catastrophic Biological Risks
Assessing Global Catastrophic Biological Risks
In this talk from EA Global 2018: San Francisco, Dr. Crystal Watson shares foundational thinking about Global Catastrophic Biological Risks, how the Center for Health Security at Johns Hopkins is working to better understand and reduce them, and how effective altruists may be able to get involved. This is a transcript of Crystal's talk, and her answers to questions from the audience, which we have lightly edited for readability.
The Talk
I'm very excited to talk to you today about what my colleagues and I have been working on to address Global Catastrophic Biological Risks, or GCBRs. I'll cover the definition that we have proposed for GCBRs, why we think they are important to work on, why you might be interested, what can be done to address these risks, and what we are doing at our center to work on them. I'll finish up by talking about what you as members of the Effective Altruism community might do, if you're interested in engaging with this topic.
The Eradication of Smallpox
Before I jump into GCBRs directly, I first want to tell you a little about how our center, the Center for Health Security, got its start. This is a classic public health story that you may already know about, which I think demonstrates the devastating power of infectious diseases, but also the power of humankind to address these types of risks. Our center was co-founded under the direction of Dr. D. A. Henderson, the leader of the World Health Organization's campaign to eradicate smallpox back in the 1970s and 80s.
Prior to 1977, when he had the last case of smallpox in nature, the disease was endemic to many parts of the world. Even when smallpox had been eliminated from some places like the United States, it was still killing about 2 million people a year before eradication began. And even in the US, as late as 1947, when there was an introduction of a case from somewhere else in the world, it was a huge problem. In 1947, there was one imported case in New York City, which resulted in just a handful of secondary cases. That exposure resulted in the vaccination of about 2.5 million people, to give an idea of what a problem this was.
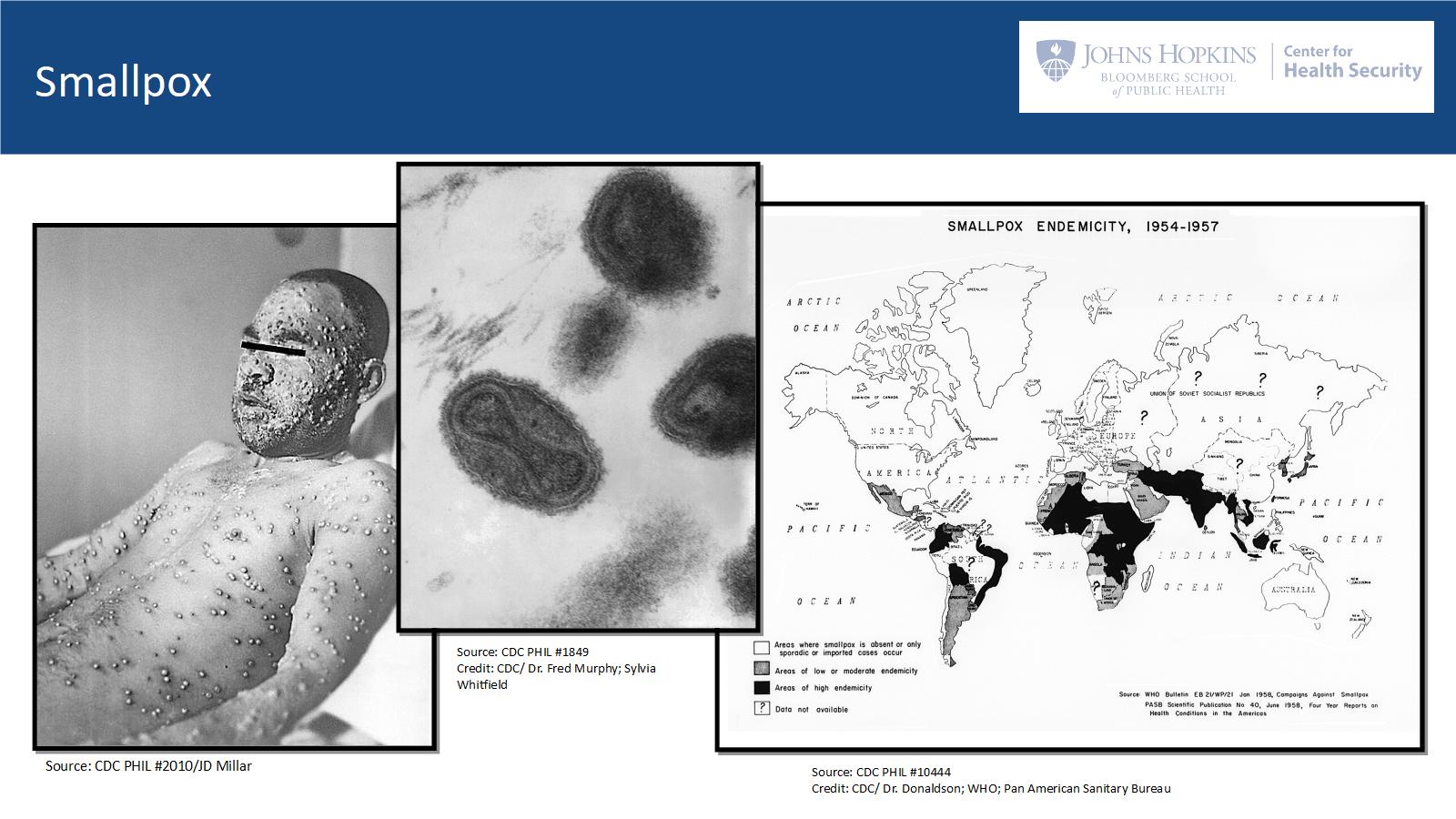
Smallpox was one of the most dreaded diseases in history. It killed about a third of the people who were infected, and those who survived where permanently scarred. As well as scarring, some survivors were blinded by the disease as well. Smallpox was particularly devastating when it was introduced into an immunologically naïve population, meaning a population that hadn't experience the virus before. For example, when smallpox - along with measles and some other childhood diseases - was introduced into the Western Hemisphere in 1492, over the next century it resulted in an epidemic that killed up to 90% of the impacted native populations, which in turn caused widespread social and economic collapse.
Fortunately, smallpox also ushered in the vaccine era, with discovery of the first vaccine by Edward Jenner. But without a vaccine, and for naïve populations, the disease could be catastrophic. So, smallpox was a terrible burden for humanity for centuries, and its eradication was one of humanity's greatest achievements. Dr. Henderson really took up the mantle of eradication when he was called upon. The program that he helped lead was a true testament to what can be done when you have excellent leadership, operational ingenuity, and some really simple tools.
When DA started his work in Geneva, smallpox was endemic to many parts of the world. The goal was to have zero cases, or "smallpox zero", as they called it. In order to reach that goal, they had to reach both some of the most densely populated areas on earth, and also some of the most remote villages that were very hard to access. And it had to be done on a shoestring budget. The estimate for the total cost of eradication was only 300 million dollars for about a 10 year program.
There were specific characteristics of the variola virus - the virus responsible for smallpox - that made it possible to eradicate. It only infected humans, meaning that there was no animal reservoir, so it didn't lurk somewhere else with the possibility of being reintroduced into the human population. It was not communicable until someone was symptomatic; if there was asymptomic spread, it would have made it more difficult to control. And we had a very effective vaccine. There was also a very simple tool that was developed during the eradication campaign, called the bifurcated needle, which is pictured here:
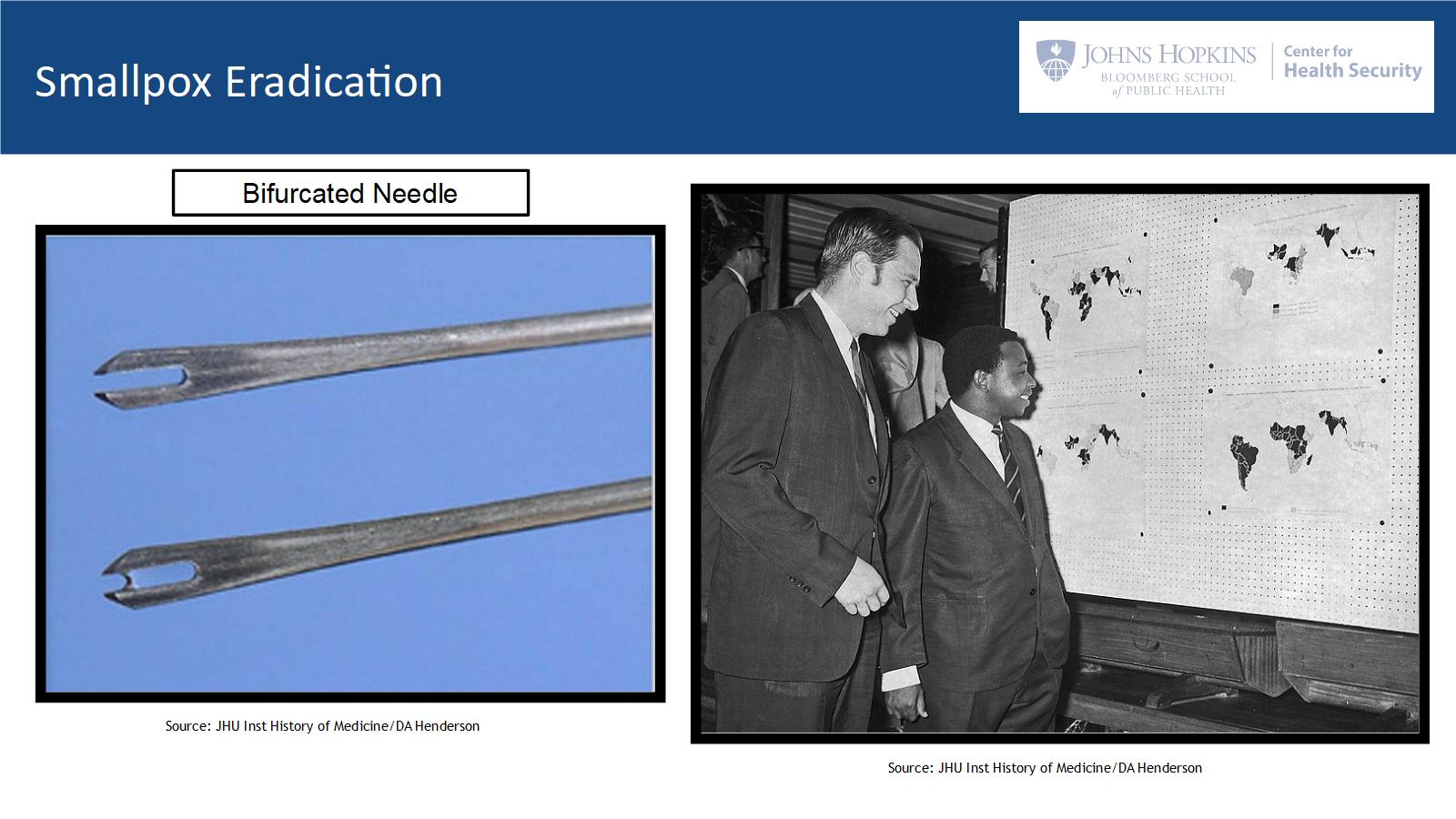
The bifurcated needle works like so: you dip the needle into some of the smallpox vaccine, and it holds that very small amount of vaccine liquid in between its prongs through capillary action. Then, the needle is used to vaccinate on an arm, by being pressed into the skin multiple times.
This application was actually very effective - enough to induce immunity, and it was also very easy to teach somebody how to administer. The ease of administration let D. A. and his team deputize people all over the world to go out and become eradicators. Tens of thousands of people in all corners of the globe were going from house to house, from village to village, giving this vaccination and helping with eradication.
The reason I start with this example is that while it demonstrates the catastrophic nature of some infectious disease emergencies, I think it also proves that humanity has the capacity to come together on a global scale, and combat these types of infectious diseases and biological threats. So I take hope from this for the future, because now we know that there are biological events that are possible that could be much worse than smallpox.
Defining Global Catastrophic Biological Risks
GCBRS are one of a few categories of risk with the potential, I think, to severely or even permanently derail humanity. Our center has been working to help define these risks, and this is just a short summary of what we think characterizes GCBRs.
They are events in which a biological agent could lead to sudden extraordinary widespread disaster. Importantly, in order for an event to be catastrophic, it would have to quickly go beyond the normal capabilities of governments and the private sector to manage it. And if totally unchecked, a GCBR would have many other devastating effects beyond just the death toll of the disease itself.
As a shorthand for catastrophic biological events we think of GCBRs as at the level of 1918 influenza pandemic and above. The 1918 flu is estimated to have killed on the order of 50 to 100 million people, which is more than were killed in all the wars of the 20th century combined.
Obviously, most biological events are not going to be catastrophic. We have a long history of epidemics and even pandemics, which were either brought under control, or just didn't have the characteristics that would make them catastrophic events. But we do think there are a handful of scenarios that could have catastrophic potential.
Specifically, we think it's conceivable that bio-warfare could be catastrophic. Globally we have a history of offensive biological weapons programs by nation states, many of which were discontinued in the 70s and the 80s. In addition, the US had a biological weapons program, which was also discontinued. But we think that there are some nations that still have biological weapons as an active focus.
Bioterrorism, particularly a series of bioterrorism attacks, has the potential to be catastrophic, depending on the agent that's used. Giving recent advancements in a synthetic biology and biotechnology, an accidental or an intentional release of an engineered pathogen could be catastrophic. There are also scenarios where ecosystems that we rely on for survival could be disrupted through biological means, which could cause, among other risks, the catastrophic elimination of a major food source.
And finally there's a possibility of a natural emergence. Of a novel, highly virulent, highly transmissible pathogen, which could be a bad day for us. So, although the probability of any one of these things happening is very small and difficult to quantify, any of these scenarios, if one were to occur, could negatively alter the course of human history. So, I think spending some time and investing some effort in combating some of these risks is important to do.
GCBR Work at the Center for Health Security
Now that I've spoken a little bit about the risks, I want to highlight some of the work that our center is doing to begin to address these problems. I should also say that there are a number of other organizations like The Future of Humanity Institute, The Cambridge Center for Existential Risk, and the Center for Catastrophic Risk that have been addressing other types of catastrophic risk, such as AI and nuclear winter, but GCBRs are still a relatively new area of study.
So, in beginning to think about these risks, our center wanted to first propose a definition, and provide examples of potential GCB events. My colleague Monica Schoch-Spana is currently working on a project looking at fine tuning that definition and also trying to find ways to communicate about these risks so that more people can get engaged and involved. My colleague Amesh Adalja just finished a project looking at the characteristics of pandemic pathogens: what would make a pathogen more likely to become a pandemic or a GCB event.
We have work going on by Dr. Gigi Gronvall, who did a red teaming exercise recently. She brought together biologists from all stages of their careers to brainstorm about how biology could be misused. That was done with the purpose of trying to improve our ability to detect and understand when something bad is going to happen in biology.
So those are the risk side of the equation. We're also working on some projects looking at how to address these risks. My colleague Caitlin Rivers is working on a project to bring epidemic modeling, and data science, more into the field of epidemic response, which doesn't always happen now. And I'm working with a team, including Caitlyn, Tara Sell and Matt Watson, to look at types of technologies that we think could be useful in either preventing or in actually responding to a serious pandemic. We're keeping in mind the gold standard of the bifurcated needle. That's what we want to do. We want to find the next bifurcated needle.
One other project that we're very proud of, which we finished last month, was called the Clade X Pandemic Exercise. We brought together senior leaders, former government officials including former Senator Tom Daschle, former CDC Director Julie Gerberding, and a former FDA commissioner, and they all came together and sat at the table and went through a catastrophic risk exercise.
We live-streamed the event, which has a lot of interesting lessons. The Clade X exercise involved the fictitious release of a genetically engineered pathogen, which was a pair influenza virus with added variance factors from a closely related virus. This combination made Clade X about as transmissible as SARS and less than influenza. Its case fatality ratio was also moderate, greater than that of 1918 flu, but much less than viruses like Ebola or H5N1 flu.
The virus in the scenario was introduced in multiple attacks around the world, and then it spread globally. The scenario progressed and eventually led to a catastrophic outcome, with more than 150 million deaths worldwide within about 18 months. Some of the key points that were highlighted in this scenario were about the need for rapid development, manufacturing and distribution of vaccine, the need for planning our responses to this kind of an event, and the need for both national and global cooperation and preparation. These are just to name a few of the issues. The stream is archived online if you're interested in going back and watching any part of the day.
We're excited to see that the Clade X exercise is already raising awareness in the US and internationally, and we're hoping it will have some more tangible impacts. We've got an indication that it may be influencing some legislation that's moving in the US House right now, which is exciting. All that being said, there is a lot more work that we need to do to reduce GCBRs. If you're interested in this topic, and you want to engage further, there's a number or ways I think that members of the EA community can engage.
How to Engage with GCBR-Mitigation
The first way to engage is through work and innovation. Finding the next bifurcated needle is a big challenge, but it could change the game for GCBRs. If you want to do research there's a number of graduate programs, some of which were highlighted on the recent 80,000 Hours podcast with our director, Tom Inglesby. We're also starting a doctoral level program at Johns Hopkins, focused on health security, and we're looking for students. Another way to contribute is to apply to an organization to donate your time or resources to help organizations who are tackling these issues.
If you don't want to do research, policy change is extremely important as well. I went into government briefly at the Federal level, and in my experience, there's a lot you can do from inside government to make changes. And finally, spreading the word about Global Catastrophic Biological Risks is always very important.
Questions
Question: Are we just getting lucky? A catastrophic pandemic hasn't happened in 100 years, but I can recall Ebola and SARS and there's always the kind of bird flu, swine flu news items running around. Is this rare or are we lucky, or how should I be thinking about that?
Crystal: I think it's a combination of luck and, sometimes, successful interventions to make these outbreaks less severe. But I do think we've seen a number of pandemics in history that have been quite devastating for humanity, and so I do think it's kind of an inevitable thing that we will see something else.
Question: Do you see danger in bringing the brain trust together, such as you did in the Clade X livestream? Is there a potential risk in just bringing people together and thinking about this in a structured way in the first place?
Crystal: Yeah, so there's not a way to classify information outside of the government space, but I think it's really important to keep in mind that there is information risk when you're talking about these things. We don't want to create a recipe for somebody to follow, to do something really terrible. We definitely keep that in mind in everything that we do. Gigi's project has some potential information risk, but she every step of the way wanted to keep that in mind and make sure that information that made the risks worse wasn't put out into the world.
Question: Can you contextualize for us what 150 million deaths looks like to the 6.85 billion of us who are still hopefully around when that happens? Does that bring us to the brink or are we resilient to that?
Crystal: I think we've seen resilience to that level of pandemic before. There are different flavors of catastrophic risk. Our center has focused on all across the spectrum, but we come from a background of doing traditional bio-security. We think it's really important to focus on these higher level risks, but I think there are some that could derail humanity, but not necessarily end humanity. But there may be some existential risks as well.
Question: Do you think there are lessons from other categories of x-risk that can be applied to Biology? You mentioned that GCBR risk analysis is a little bit newer, but they're all pretty new. Are there things that you can draw from, say, the AI research field to apply to your work?
Crystal: Yeah, I think GCBRs are so new that even just taking the time to sit down and think about them in a systematic way is a good start. I'm sure there are many other lessons that can be learned from existential risk research, but we're basically at the definition stage with GCBRs. We have a lot of work to do.
Question: Are there any particularly compelling platforms, systems, technologies in the space of pandemic preparedness that you think would be worth highlighting for the audience as early things to familiarize themselves with?
Crystal: Yeah, so we've just done this project looking at technologies that we think could be helpful. There's a number of technologies that I think are potentially game changing. For example, although there's a lot of risk potentially with Synthetic Biology, it is one of our best tools to combat these issues. So, using Synthetic Biology - doing distributed manufacturing of medical countermeasures - could be something that changes the game when we need to respond to something bad. There'll be a lot more information in our report coming out, so I don't want to go into too much depth, but I think that's one area of needed investment.